
Abstract
Summary
Eighty children with nephrotic syndrome underwent lumbar spine densitometry and vertebral morphometry soon after glucocorticoid initiation. We found an inverse relationship between glucocorticoid exposure and spine areal bone mineral density (BMD) Z-score and a low rate of vertebral deformities (8%).
Introduction
Vertebral fractures are an under-recognized complication of childhood glucocorticoid-treated illnesses. Our goal was to study the relationships among glucocorticoid exposure, lumbar spine areal BMD (LS BMD), and vertebral shape in glucocorticoid-treated children with new-onset nephrotic syndrome.
Methods
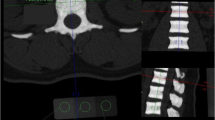
Lateral thoracolumbar spine radiography and LS BMD were performed in 80 children with nephrotic syndrome (median age 4.4 years; 46 boys) within the first 37 days of glucocorticoid therapy. Genant semiquantitative grading was used as the primary method for vertebral morphometry; the algorithm-based qualitative (ABQ) method was used for secondary vertebral deformity analysis.
Results
Six of the 78 children with usable radiographs (8%; 95% confidence interval 4 to 16%) manifested a single Genant grade 1 deformity each. All deformities were mild anterior wedging (two at each of T6, T7, and T8). Four of the 78 children (5%; 95% confidence interval 2 to 13%) showed one ABQ sign of fracture each (loss of endplate parallelism; two children at T6 and two at T8). Two of the children with ABQ signs also had a Genant grade 1 deformity in the same vertebral body. None of the children with a Genant or ABQ deformity reported back pain. An inverse relationship was identified between LS BMD Z-score and glucocorticoid exposure.
Conclusions
Although we identified an inverse relationship between steroid exposure and LS BMD soon after glucocorticoid initiation for childhood nephrotic syndrome, there was only a low rate of vertebral deformities. The clinical significance of these findings requires further study.

Similar content being viewed by others


Abbreviations
- ABQ:
-
Algorithm-based qualitative
- BMI:
-
Body Mass Index
- BMD:
-
Bone mineral density
- CI:
-
Confidence interval
- GC:
-
Glucocorticoid
- LS:
-
Lumbar spine
- NS:
-
Nephrotic syndrome
References
Schlesinger ER, Sultz HA, Mosher WE, Feldman JG (1968) The nephrotic syndrome. Its incidence and implications for the community. Am J Dis Child 116:623–632
Hodson EM, Knight JF, Willis NS, Craig JC (2001) Corticosteroid therapy for nephrotic syndrome in children. Cochrane Database Syst Rev 2
Clark AG, Barratt TM (1999) Steroid-responsive nephrotic syndrome. In: Barratt TM, Avner ED, Harmon WE (eds) Pediatric nephrology, 4th edn. Lippincott, Hagerstown
van Staa TP, Cooper C, Leufkens HG, Bishop N (2003) Children and the risk of fractures caused by oral corticosteroids. J Bone Miner Res 18:913–918
Dalle Carbonare L, Arlot ME, Chavassieux PM, Roux JP, Portero NR, Meunier PJ (2001) Comparison of trabecular bone microarchitecture and remodeling in glucocorticoid-induced and postmenopausal osteoporosis. J Bone Miner Res 16:97–103
Canalis E, Mazziotti G, Giustina A, Bilezikian JP (2007) Glucocorticoid-induced osteoporosis: pathophysiology and therapy. Osteoporos Int 18:1319–1328
Lukert BP (1992) Glucocorticoid-induced osteoporosis. South Med J 85(2):S48–S51
Ruegsegger P, Medici TC, Anliker M (1983) Corticosteroid-induced bone loss. A longitudinal study of alternate day therapy in patients with bronchial asthma using quantitative computed tomography. Eur J Clin Pharmacol 25:615–620
Bak M, Serdaroglu E, Guclu R (2006) Prophylactic calcium and vitamin D treatments in steroid-treated children with nephrotic syndrome. Pediatr Nephrol 21:350–354
Acott PD, Wong JA, Lang BA, Crocker JF (2005) Pamidronate treatment of pediatric fracture patients on chronic steroid therapy. Pediatr Nephrol 20:368–373
Leonard MB, Feldman HI, Shults J, Zemel BS, Foster BJ, Stallings VA (2004) Long-term, high-dose glucocorticoids and bone mineral content in childhood glucocorticoid-sensitive nephrotic syndrome. N Engl J Med 351:868–875
Sbrocchi AM, Rauch F, Matzinger M, Feber J, Ward LM (2010) Vertebral fractures despite normal spine bone mineral density in a boy with nephrotic syndrome. Pediatr Nephrol 26:139–142
Institute of Medicine (1997) Dietary reference intakes for calcium, phosphorus, magnesium, vitamin D, fluoride. National Academy Press, Washington
Ogden CL, Kuczmarski RJ, Flegal KM, Mei Z, Guo S, Wei R, Grummer-Strawn LM, Curtin LR, Roche AF, Johnson CL (2002) Centers for Disease Control and Prevention 2000 growth charts for the United States: improvements to the 1977 National Center for Health Statistics version. Pediatrics 109:45–60
World Health Organization Multicentre Growth Reference Study Group (2006) WHO Child Growth Standards: length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: methods and development. World Health Organization, Geneva, pp 229–300
Marshall WA, Tanner JM (1969) Variations in pattern of pubertal changes in girls. Arch Dis Child 44:291–303
Marshall WA, Tanner JM (1970) Variations in the pattern of pubertal changes in boys. Arch Dis Child 45:13–23
Musgrave KO, Giambalvo L, Leclerc HL, Cook RA, Rosen CJ (1989) Validation of a quantitative food frequency questionnaire for rapid assessment of dietary calcium intake. J Am Diet Assoc 89:1484–1488
Halton J, Gaboury I, Grant R et al (2009) Advanced vertebral fracture among newly diagnosed children with acute lymphoblastic leukemia: results of the Canadian Steroid-Associated Osteoporosis in the Pediatric Population (STOPP) research program. J Bone Miner Res 24:1326–1334
Public Health Agency of Canada. Canada's physical activity guide for children. http://www.phac-aspc.gc.ca/hp-ps/hl-mvs/pag-gap/cy-ej/children-enfants/index-eng.php. Accessed 31 March 2010
van Staa TP, Leufkens HG, Cooper C (2002) The epidemiology of corticosteroid-induced osteoporosis: a meta-analysis. Osteoporos Int 13:777–787
Curtis JR, Westfall AO, Allison J, Bijlsma JW, Freeman A, George V, Kovac SH, Spettell CM, Saag KG (2006) Population-based assessment of adverse events associated with long-term glucocorticoid use. Arthritis Rheum 55:420–426
Dubner SE, Shults J, Baldassano RN, Zemel BS, Thayu M, Burnham JM, Herskovitz RM, Howard KM, Leonard MB (2009) Longitudinal assessment of bone density and structure in an incident cohort of children with Crohn's disease. Gastroenterology 136:123–130
Genant HK, Wu CY, van Kuijk C, Nevitt MC (1993) Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res 8:1137–1148
Keats TE, Smith TH (1977) An atlas of normal developmental anatomy. Year book of medical publishers, 2nd Ed. Chicago
Jiang G, Eastell R, Barrington NA, Ferrar L (2004) Comparison of methods for the visual identification of prevalent vertebral fracture in osteoporosis. Osteoporos Int 15:887–896
Newcombe RG (1998) Two-sided confidence intervals for the single proportion: comparison of seven methods. Stat Med 17:857–872
Fujita T, Satomura A, Hidaka M, Ohsawa I, Endo M, Ohi H (2000) Acute alteration in bone mineral density and biochemical markers for bone metabolism in nephrotic patients receiving high-dose glucocorticoid and one-cycle etidronate therapy. Calcif Tissue Int 66:195–199
Cohen A, Shane E (2003) Osteoporosis after solid organ and bone marrow transplantation. Osteoporos Int 14:617–630
Wetzsteon RJ, Shults J, Zemel BS, Gupta PU, Burnham JM, Herskovitz RM, Howard KM, Leonard MB (2009) Divergent effects of glucocorticoids on cortical and trabecular compartment bone mineral density in childhood nephrotic syndrome. J Bone Miner Res 24(3):503–513
Hegarty J, Mughal MZ, Adams J, Webb NJ (2005) Reduced bone mineral density in adults treated with high-dose corticosteroids for childhood nephrotic syndrome. Kidney Int 68:2304–2309
Dennison E, Cooper C (2000) Epidemiology of osteoporotic fractures. Horm Res 54(Suppl 1):58–63
Valta H, Lahdenne P, Jalanko H, Aalto K, Makitie O (2007) Bone health and growth in glucocorticoid-treated patients with juvenile idiopathic arthritis. J Rheumatol 34:831–836
Gaca AM, Barnhart HX, Bisset GS 3rd (2010) Evaluation of wedging of lower thoracic and upper lumbar vertebral bodies in the pediatric population. AJR Am J Roentgenol 194:516–520
Ebel KD, Blickman H, Willich E, Richter E (1999) Abnormalities in vertebral body shape and size. Differential diagnosis in pediatric radiology. Thieme Publishers, NY
Rea JA, Chen MB, Li J, Blake GM, Steiger P, Genant HK, Fogelman I (2000) Morphometric X-ray absorptiometry and morphometric radiography of the spine: a comparison of prevalent vertebral deformity identification. J Bone Miner Res 15:564–574
Vallarta-Ast N, Krueger D, Wrase C, Agrawal S, Binkley N (2007) An evaluation of densitometric vertebral fracture assessment in men. Osteoporos Int 18:1405–1410
Wu C, van Kuijk C, Li J, Jiang Y, Chan M, Countryman P, Genant HK (2000) Comparison of digitized images with original radiography for semiquantitative assessment of osteoporotic fractures. Osteoporos Int 11:25–30
Jackson SA, Tenenhouse A, Robertson L (2000) Vertebral fracture definition from population-based data: preliminary results from the Canadian Multicenter Osteoporosis Study (CaMos). Osteoporos Int 11:680–687
Huber A, Gaboury I, Cabral DA et al (2010) Prevalent vertebral fractures among children initiating glucocorticoid therapy for the treatment of rheumatic disorders. Arthitis Care Res (Hoboken) 62:516–526
Ismail AA, Cooper C, Felsenberg D, Varlow J, Kanis JA, Silman AJ, O'Neill TW (1999) Number and type of vertebral deformities: epidemiological characteristics and relation to back pain and height loss. European Vertebral Osteoporosis Study Group. Osteoporos Int 9:206–213
Delmas PD, Genant HK, Crans GG, Stock JL, Wong M, Siris E, Adachi JD (2003) Severity of prevalent vertebral fractures and the risk of subsequent vertebral and nonvertebral fractures: results from the MORE trial. Bone 33:522–532
Peel NF, Moore DJ, Barrington NA, Bax DE, Eastell R (1995) Risk of vertebral fracture and relationship to bone mineral density in steroid treated rheumatoid arthritis. Ann Rheum Dis 54:801–806
Dubner SE, Shults J, Leonard MB, Zemel BS, Sembhi H, Burnham JM (2008) Assessment of spine bone mineral density in juvenile idiopathic arthritis: impact of scan projection. J Clin Densitom 11:302–308
Acknowledgments
This study was primarily funded by an operating grant from the Canadian Institutes for Health Research. Additional funding for this work has been provided by the Canadian Institutes for Health Research New Investigator Program (to Dr. Leanne Ward), the Canadian Child Health Clinician Scientist Career Enhancement Program (to Dr. Leanne Ward), the Children's Hospital of Eastern Ontario, and Women and Children's Health Research Institute, University of Alberta.
In addition, the Canadian STOPP Consortium would like to thank the following individuals who contributed to the study: The children and their families who participated in the study, making the STOPP research program possible; the research associates who managed the study at the coordinating center (the Children's Hospital of Eastern Ontario Ottawa, Ontario): Elizabeth Sykes (STOPP project manager), Maya Scharke (STOPP data analyst and database manager), Monica Tomiak (statistical analyses), Victor Konji (STOPP publications and presentations committee liaison and hand morphometry measurements), Steve Anderson (Children's Hospital of Eastern Ontario, Pediatric Bone Health Program research manager), Catherine Riddell (STOPP national study monitor); and research associates who took care of the patients from the following institutions: Alberta Children's Hospital, Calgary, Alberta—Eileen Pyra; British Columbia Children's Hospital, Vancouver British Columbia—Terry Viczko, Sandy Hwang; Children's Hospital of Eastern Ontario, Ottawa, Ontario—Heather Cosgrove, Amanda George, Josie MacLennan, Catherine Riddell; Children's Hospital of Western Ontario, London, Ontario—Leila MacBean, Mala Ramu; McMaster Children's Hospital, Hamilton, Ontario—Susan Docherty-Skippen; IWK Health Center, Halifax, Nova Scotia—Aleasha Warner; Montréal Children's Hospital, Montréal, Québec—Diane Laforte, Maritza Laprise, Mayito St-Pierre; Ste. Justine Hospital, Montréal, Québec—Claude Belleville, Stéphanie Pellerin, Natacha Gaulin Marion; Stollery Children's Hospital, Edmonton, Alberta—Deborah Olmstead, Melissa Gabruck, Linda Manasterski; Toronto Hospital for Sick Children, Toronto, Ontario—Julie Lee, Karen Whitney; Winnipeg Children's Hospital, Winnipeg, Manitoba—Dan Catte, Erika Bloomfield. The research nurses, support staff, and all the STOPP collaborators from the various Divisions of Nephrology, Oncology, Rheumatology, and Radiology have contributed to the care of the children enrolled in the study.
Funding
The primary funding source is the Canadian Institutes of Health Research. Additional funding sources are from the Canadian Child Health Clinician Scientist Program; the Children's Hospital of Eastern Ontario Research Institute and Departments of Pediatrics and Surgery; and the Women and Children's Health Research Institute, University of Alberta.
Conflicts of Interest
None.
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
About this article
Cite this article
Feber, J., Gaboury, I., Ni, A. et al. Skeletal findings in children recently initiating glucocorticoids for the treatment of nephrotic syndrome. Osteoporos Int 23, 751–760 (2012). https://doi.org/10.1007/s00198-011-1621-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-011-1621-2