
Abstract
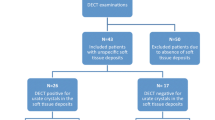
The aim of the study was to investigate the sensitivity and specificity of dual-energy computed tomography in the diagnosis of acute gouty arthritis, and the related risk factors for urate crystal deposition. One hundred ninety-one patients (143 with acute gouty arthritis and 48 with other arthritic conditions) were studied. All patients had acute arthritic attack in the recent 15 days and underwent dual-energy computed tomography (DECT) scan with the affected joints. The urate volume was calculated by DECT and the basic information of these patients was recorded at the same time. Uric acid crystals were identified with DECT in 140 of 143 (97.9 %) gout patients and 6 of 48 (12.5 %) of nongout patients, respectively. The sensitivity, specificity, positive predictive value, and negative predictive value of DECT in the diagnosis of acute gouty arthritis were 97.9, 87.5, 95.9, and 93.3 %, respectively. The urate volumes were ranged from 0.57 to 54,543.27 mm3 with a mean volume of 1,787.81 ± 7,181.54 mm3. Interestingly, urate volume was correlated with the disease duration, serum uric acid levels, the presence of tophi, and bone erosion. Two-year follow-up data was available in one patient with recurrent gouty arthritis, whose urate volume was gradually reduced in size by DECT detection after urate-lowering therapies. DECT showed high sensitivity and specificity for the identification of urate crystals and diagnosis of acute gout. The risk factors for uric acid deposition include the disease duration, serum uric acid levels, the presence of tophi, and bone erosion. DECT has an important role in the differential diagnosis of arthritis, and also could be served as a follow-up tool.



Similar content being viewed by others


References
Zhu Y, Pandya BJ, Choi HK (2011) Prevalence of gout and hyperuricemia in the US general population: the National Health and Nutrition Examination Survey 2007-2008. Arthritis Rheum 63(10):3136–3141
Whelton A, MacDonald PA, Chefo S, Gunawardhana L (2013) Preservation of renal function during gout treatment with febuxostat: a quantitative study. Postgrad Med 125(1):106–114
Kelkar A, Kuo A, Frishman WH (2011) Allopurinol as a cardiovascular drug. Cardiol Rev 19(6):265–271
Kim HR, Lee JH, Oh J, Kim NR, Lee SH (2012) Clinical images: detection of gouty arthritis in the atlantoaxial joint using dual-energy computed tomography. Arthritis Rheum 64(4):1290
Dalbeth N, Choi HK (2013) Dual-energy computed tomography for gout diagnosis and management. Curr Rheumatol Rep 15(1):301
Wallace SL, Robinson H, Masi AT, Decker JL, McCarty DJ, Yü TF (1977) Preliminary criteria for the classification of the acute arthritis of primary gout. Arthritis Rheum 20(3):895–900
Graf SW, Buchbinder R, Zochling J, Whittle SL (2013) The accuracy of methods for urate crystal detection in synovial fluid and the effect of sample handling: a systematic review. Clin Rheumatol 32(2):225–232
Malik A, Schumacher HR, Dinnella JE, Clayburne GM (2009) Clinical diagnostic criteria for gout: comparison with the gold standard of synovial fluid crystal analysis. J Clin Rheumatol 15(1):22–24
McQueen FM, Doyle A, Dalbeth N (2011) Imaging in gout—what can we learn from MRI, CT, DECT and US? Arthritis Res Ther 13(6):246
Choi HK, Al-Arfaj AM, Eftekhari A, Munk PL, Shojania K, Reid G, Nicolaou S (2009) Dual energy computed tomography in tophaceous gout. Ann Rheum Dis 68(10):1609–1612
Bacani AK, McCollough CH, Glazebrook KN, Bond JR, Michet CJ, Milks J, Manek NJ (2012) Dual energy computed tomography for quantification of tissue urate deposits in tophaceous gout: help from modern physics in the management of an ancient disease. Rheumatol Int 32(1):235–239
Dalbeth N, Kalluru R, Aati O, Horne A, Doyle AJ, McQueen FM (2013) Tendon involvement in the feet of patients with gout: a dual-energy CT study. Ann Rheum Dis 72(9):1545–1548
Dalbeth N, Aati O, Gao A, House M, Liu Q, Horne A, Doyle A, McQueen FM (2012) Assessment of tophus size: a comparison between physical measurement methods and dual-energy computed tomography scanning. J Clin Rheumatol 18(1):23–27
Desai MA, Peterson JJ, Garner HW, Kransdorf MJ (2011) Clinical utility of dual-energy CT for evaluation of tophaceous gout. Radiographics 31(5):1365–1375
Choi HK, Burns LC, Shojania K (2012) Dual energy CT in gout: a prospective validation study. Ann Rheum Dis 71(9):1466–1471
Glazebrook KN, Guimarães LS, Murthy NS, Black DF, Bongartz T, Manek NJ, Leng S, Fletcher JG, McCollough CH (2011) Identification of intraarticular and periarticular uric acid crystals with dual-energy CT: initial evaluation. Radiology 261(2):516–524
Nicolaou S, Yong-Hing CJ, Galea-Soler S, Hou DJ, Louis L, Munk P (2010) Dual-energy CT as a potential new diagnostic tool in the management of gout in the acute setting. Am J Roentgenol 194(4):1072–1078
Kim SK, Lee H, Kim JH, Park SH, Lee SK, Choe JY (2013) Potential interest of dual-energy computed tomography in gout: focus on anatomical distribution and clinical association. Rheumatology 52(2):402–403
Dalbeth N, Clark B, Gregory K, Gamble G, Sheehan T, Doyle A, McQueen FM (2009) Mechanisms of bone erosion in gout: a quantitative analysis using plain radiography and computed tomography. Ann Rheum Dis 68(8):1290–1295
Manger B, Lell M, Wacker J, Schett G, Rech J (2012) Detection of periarticular urate deposits with dual energy CT in patients with acute gouty arthritis. Ann Rheum Dis 71(3):470–471
Acknowledgments
This work was supported by Dr. Liang Zhu, MD, Department of Rheumatology, Second affiliated hospital, School of medicine, Zhejiang University, Hangzhou, China, who revised the data. It was also supported by Dr. Risheng Yu, Department of Radiology, Second affiliated hospital, School of medicine, Zhejiang University, Hangzhou, China.
Disclosures
All authors declare that they have no conflicts of interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Wu, H., Xue, J., Ye, L. et al. The application of dual-energy computed tomography in the diagnosis of acute gouty arthritis. Clin Rheumatol 33, 975–979 (2014). https://doi.org/10.1007/s10067-014-2606-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-014-2606-2