
Abstract
Environmental factors play an important role in the development of rheumatoid arthritis (RA). Among these factors, smoking is generally considered to be an established risk factor for RA. Data regarding the impact of diet on risk of RA development is limited. This study assessed the impact of dietary patterns on RA susceptibility in Chinese populations. This was a large scale, case-control study composed of 968 patients with RA and 1037 matched healthy controls. Subjects were recruited from 18 teaching hospitals. Socio-demographic characteristics and dietary intakes 5 years prior to the onset of RA were reported by a self-administered questionnaire. Differences in quantity of consumption between cases and controls were analyzed by Student’s t test. Multiple logistic regression analysis was applied to identify independent dietary risk factor(s) responsible for RA susceptibility. Compared to healthy individuals, RA patients had decreased consumption of mushrooms (P = 0.000), beans (P = 0.006), citrus (P = 0.000), poultry (P = 0.000), fish (P = 0.000), edible viscera (P = 0.018), and dairy products (P = 0.005). Multivariate analyses revealed that several dietary items may have protective effects on RA development, such as mushrooms (aOR = 0.669; 95%CI = 0.518–0.864, P = 0.002), citrus fruits (aOR = 0.990; 95%CI = 0.981–0.999, P = 0.04), and dairy products (aOR = 0.921; 95%CI 0.867–0.977, P = 0.006). Several dietary factors had independent effects on RA susceptibility. Dietary interventions may reduce the risk of RA.
Similar content being viewed by others

Introduction
Rheumatoid arthritis (RA) is a chronic systemic inflammatory disease that leads to progressive joint erosion and destruction and affects 0.5–1 % of the population. RA is considered to be a complex disease that is triggered by both genetic and environmental factors, and the pathogenesis of RA has not yet been fully elucidated. Recent advances in high-throughput genome scanning have enabled the identification of many genetic risk factors that contribute to RA susceptibility. However, it has been estimated that the genetic factors account for only 60 % of the risk for RA susceptibility [1], while environmental and other non-genetic factors account for the remaining 40 %.
Among environmental factors, while only smoking is currently considered to be an established risk factor for RA [2, 3], other factors, such as diet, may contribute to RA susceptibility. Diet is an environmental factor that affects inflammation, antigen presentation, antioxidant defense mechanisms, allergies, and gut microbiota, and the exact impact of diet on RA risk remains uncertain. Several case-control studies have suggested that omega-3 fatty acids, which are present in fish, soybean, safflower, sunflower, and corn oils, may confer protection against RA [4, 5]. Alcohol may reduce the risk of RA in women [6]. While reactive oxygen species (ROS) are produced in rheumatoid joints [7], the roles of dietary factors such as antioxidants and vitamins in the pathogenesis of RA remain unclear. Vitamin C is both an intracellular and an extracellular scavenger of ROS, and in models of rat adjuvant arthritis supplementation with vitamin C contributed to improved arthritis scores, evidenced by a reduction in paw volume [8, 9]. However, there is little clinical evidence on the effects of antioxidants, such as vitamins E and C, on individuals with RA [10, 11]. A 2-year study on the effects of the Mediterranean diet on RA patients revealed that the consumption of cereals, vegetables, legumes, fruits, and olive oil decreased the risk of new onset of inflammatory polyarthritis [12].
While there is evidence on the effects of diet on RA pathogenesis in Western populations, there is little information to date concerning the impact of diet on the development of RA in Chinese populations. Here, we assess the impact of dietary factors on the development of RA in Chinese populations.
Patients and methods
Study population
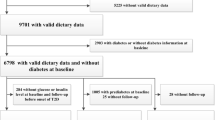
A total of 968 RA patients and 1037 ethnic and geographically matched healthy controls were recruited from 18 hospitals (Fig. 1). All RA patients fulfilled the American College of Rheumatology (ACR) criteria for RA [13]. Healthy controls were randomly selected from medical workers without any history of chronic diseases. A self-administered food frequency questionnaire (FFQ) was designed to measure socio-demographic characteristics and dietary intakes. Patients were asked to complete a detailed weekly retrospective FFQ (i.e., over the last 5 years prior to RA onset). Healthy controls were required to complete a similar weekly retrospective FFQ, to gather information on their dietary intakes for the previous 5 years. FFQs were coded and analyzed. The patients and healthy controls with incomplete data from FFQs were excluded from the study.

Patient flow chart. RA rheumatoid arthritis, HC healthy controls. A total of 968 RA patients and 1037 healthy controls were recruited from 18 hospitals
The study was conducted in China between May 2012 and September 2013. A survey was designed following the guidelines established by the Chinese Rheumatology Association (CRA). The study was approved by the Medical Ethics Committee of Peking University People’s Hospital. Informed written consent forms were obtained from all study participants.
Demographic data
Demographics and personal characteristics were gathered, including gender, age, marital status, education, occupation, personal income, height, and weight.
Dietary assessment
Dietary assessment on the FFQ includes the frequency and the amount of dietary intake. The frequency of red meat, poultry, fish, edible viscera, vegetables, potatoes, mushrooms, beans, nuts, milk or yogurt, eggs, citrus, and other fruit except for citrus was measured with a response range from 1 to 8 (1 = less than once per month, 2 = 1–3 times per month, 3 = 1–2 times per week, 4 = 3–4 times per week, 5 = 5–6 times per week, 6 = 1 time per day, 7 = 2 times per day, and 8 = 3 or more times per day). The intake amount per serving of rice, flour meal, red meat, poultry, fish, edible viscera, vegetables, potatoes, mushrooms, beans, and nuts was measured with a response range from 1 to 4 (1 = 50 g or less, 2 = 50–100 g, 3 = 100–150 g, 4 = 150–200 g or more). The amount of eggs, citrus, and other fruit except for citrus was measured with a response range from 1 to 5 (1 = 1/2 or less, 2 = 1/2–2/3, 3 = 2/3–1, 4 = 1–2, 5 = 2–3 or more). The intake amount per serving of milk or yogurt was measured with a response range from 1 to 5 (1 = 50 ml or less, 2 = 50–75 ml, 3 = 75–100 ml, 4 = 100–200 ml, 5 = 200–300 ml or more). The total amount of dietary intake per month of a food item is equal to the intake amount per serving of that food item × the frequency of dietary intake.
Statistical analyses
Differences in quantity of consumption between cases and controls were assessed using t test analyses. Multiple logistic regression analysis was applied to identify independent dietary risk factor(s) responsible for RA susceptibility. Odds ratios (ORs) with 95 % confidence intervals (CIs) were calculated to estimate the relative risk. P values less than 0.05 were considered significant.
Results
Demographic profile of RA patients
The study subjects were mainly recruited from two ethnic groups: Han (n = 913) and Hui (n = 18). Additionally, there were 37 subjects coming from other ethnic groups, including Man (n = 27), Mongol (n = 7), Yi (n = 1), and Zhuang (n = 1). The demographic characteristics of patients and controls are shown in Table 1.
Dietary intakes in RA patients and healthy controls
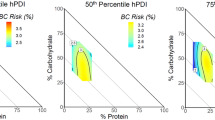
The results of the dietary intakes of both groups are shown in Fig. 2 and Table 2. Compared with healthy controls, RA patients consumed lower amounts of chicken (P = 0.0001), fish (P = 0.0001), mushrooms (P = 0.0001), beans (P = 0.006), dairy products (P = 0.005), citrus fruits (P = 0.000), and organ meats (P = 0.018). There were no significant differences in consumption of red meat between RA patients and healthy controls.

Dietary intakes of RA patients and healthy controls (HC). Compared with healthy controls, RA patients had higher amount of consumption in potatoes and lower amount of consumption in chicken, fish, mushrooms, beans, dairy products, citrus fruits, and organ meats. There were no significant differences in consumption of red meat between RA patients and healthy controls
Comparison of dietary intake between Han and Hui populations in both RA and HC groups
We compared the dietary consumption between the Han and Hui populations in the RA and HC cohorts, respectively. As shown in Table 3, except for dairy products, there were no significant differences in dietary consumption between Han and Hui groups.
Comparison of dietary intakes between Han and non-Han in both RA and HC groups
We compared the dietary consumption between the Han and non-Han populations in both RA and HC groups. Han people with RA intake more fish and less dairy products than non-Han people with RA. There were no other significant differences in dietary consumption between the Han and non-Han groups (Table 4).
Dietary intake as independent risk factor for RA development
The multivariate analyses revealed that females and individuals older than 50 years of age were more susceptible to RA (Table 5). Consumption of several dietary items were independent factors for higher risk of RA development, including potatoes (OR = 1.160; 95 % CI = 1.035–1.300, P = 0.011) and fruits except for citrus fruits (OR = 1.013; 95 % CI = 1.003–1.023, P = 0.013). In contrast, some dietary items were found to have protective effects on RA, including mushrooms (OR = 0.669; 95 % CI = 0.518–0.864, P = 0.002), dairy products (OR = 0.921; 95 % CI = 0.867–0.977, P = 0.006), and citrus fruits (OR = 0.990; 95 % CI = 0.981–0.999, P = 0.040). Consumption of red meats, fruits, and vegetables was not found to have any effect on RA risk. The analyses revealed that higher intakes of carbohydrates and lower intakes of dairy products, mushrooms, and citrus fruits may associate with RA development. There was a trend for high intakes of fish (OR = 0.864; 95%CI = 0.647–1.156, P = 0.325) and beans (OR = 0.938; 95%CI = 0.811–1.086, P = 0.391) to have protective effects against RA, though these did not reach statistical significance. Additionally, no significant associations were observed between the consumption of red meat and RA risk.
Discussion
The etiology of RA remains an area of considerable interest. RA is triggered by genetic factors; however, environmental factors may also play a role in the pathogenesis of RA. Dietary and lifestyle factors (e.g., smoking) [2, 3] contribute to RA. Smoking is so far the most well-established environmental risk factor for development of RA [2, 3]. Additionally, infectious agents such as viruses, bacteria, and fungi have long been suspected risk factors for RA, but there is no conclusive evidence to support the hypothesis [14]. Influences of other environmental factors on RA, such as hormones, have also been suggested. Hormones are believed to influence RA based on the fact that females are more prone to develop RA than are men, with a peak onset at 50–60 years of age [1, 15].
Salminen et al. [15] reported that 33–75 % patients believe that food plays an important role in their symptom severity and approximately 50 % will have tried dietary manipulation in an attempt to improve their symptoms. Diets rich in fiber, omega-3 fatty acids, and antioxidants, and low in red meat have been reported associated with decreased RA risks [16–18]. Comparing with the survey by others [16–18], Chinese diets are characterized by higher levels of vegetables and lower intakes of red meat consumption and the average meat consumption is much lower than Western diets. In this study, there were no significant differences in red meat intakes between RA patients and healthy controls, as reported in other studies [19, 20]. Whether the association between red meat consumption and inflammatiory arthritis remains unclear, meat consumption might affect the gut microbiota or contribute to high energy intakes, which provide some explanation for the association.
The results of this study revealed that high intakes of carbohydrates (e.g., potatoes) might be associated with increased RA risks. High carbohydrate and lower fiber intakes lead to excess energy intake. With excess energy intake and reduced energy expenditure, body weight and adiposity increase. Although there was no signifcant difference in body mass index (BMI) between RA patients and HCs in present work, other studies have reported that BMI is positively correlated with chronic inflammatory disorders [21]. It is recognized that adipocytes release the proinflammatory cytokines TNF, IL-1β and IL-6; thus, adipose tissue is metabolically active and contribute to sysytemic inflammatory responses [3, 21].
Studies have reported that ROS are involved in the pathogenesis of RA. Antioxidant-rich diets have beneficial effects on several diseases. However, in this study, high intakes of fruits or vegetables had no significant effects. Interestingly, citrus fruits have a protective role in the pathogenesis of RA. Citrus fruits are rich in hesperidin. Kawaguchi [22] reported that the consumption of citrus flavanone and naringin suppressed the inflammatory responses in collagen-induced arthritis in mice, possibly by decreasing tumor necrosis factor-α (TNF-α) levels. In an 8-week, placebo-controlled, randomized, double-blind clinical trial, Oben et al. reported that citrus extracts improved knee joint pain and flexibility and reduced C-reactive protein levels [23]. In addition to hesperidin and naringin, citrus fruits are rich in vitamin C, which has protective roles according to some studies and no clinical benefits according to other studies [11].
Mushroom consumption was significantly lower in RA patients than in healthy controls. Mushrooms have food and pharmaceutical applications due to the presence of β-glucans, polysaccharopeptides, and polysaccharide-protein conjugates, which have immunomodulatory and antitumor activities. These compounds have demonstrated mitogenicity and activation of immune effector cells, such as lymphocytes, macrophages, and natural killer cells, resulting in the production of cytokines, including interleukins, TNF-α, and interferon gamma [24]. Yu et al. reported that mushrooms regulate immunity in vitro [25]. A number of mushroom components have been shown to modulate immunity and therefore might play a role in preventing RA.
In this study, there were no significant benefits from fish consumption; however, fish contains omega-3 fatty acids, which have protective roles. More than 20 randomized controlled trials have reported that omega-3 fatty acids have modest benefits on RA treatment. Additionally, symptoms got worse in RA patients who discontinued the fish oil supplements [16, 26, 27].
Dairy products, such as milk and yogurt, had protective roles against RA in this study. Yogurt contains probiotics, which maintain a healthy gut microbiota. A metagenomic approach using Illumina sequencing of pooled milk samples revealed that the genera and types of bacteria in milk may affect bacterial establishment and stability in this food matrix [28]. Supplementation with Lactobacillus casei improves the inflammatory status of patients with RA [29]. A 3-month, double-blind, placebo-controlled study reported considerable improvements in RA patients following supplementation with Lactobacillus rhamnosus and Lactobacillus reuteri [30]. Additionally, the administration of probiotics in different animal models improved inflammatory bowel disease, atopic dermatitis, and RA, probably as a result of enrichment of CD4+Foxp3+ Tregs in inflamed body areas [31]. Therefore, probiotics are recommended to patients with RA.
In conclusion, dietary factors contribute to the development of RA. Dietary modification might reduce RA risk and prevent disease progression. There is a need for large-scale prospective, placebo-controlled studies to assess the effects of multiple dietary compounds on RA.
References
Liao KP, Alfredsson L, Karlson EW (2009) Environmental influences on risk for rheumatoid arthritis. Curr Opin Rheumatol 21:279–283
Di Giuseppe D, Discacciati A, Orsini N, et al. (2014) Cigarette smoking and risk of rheumatoid arthritis: a dose-response meta-analysis. Arthritis Res Ther 16:R61
de Hair MJ, Landewe RB, van de Sande MG, et al. (2013) Smoking and overweight determine the likelihood of developing rheumatoid arthritis. Ann Rheum Dis 72:1654–1658
Galli C, Calder PC (2009) Effects of fat and fatty acid intake on inflammatory and immune responses: a critical review. Ann Nutr Metab 55:123–139
Karlson EW, Mandl LA, Aweh GN, et al. (2003) Coffee consumption and risk of rheumatoid arthritis. Arthritis Rheum 48:3055–3060
Lu B, Solomon DH, Costenbader KH, et al. (2014) Alcohol consumption and risk of incident rheumatoid arthritis in women: a prospective study. Arthritis Rheumatol 66:1998–2005
Hu F, Mu R, Zhu J, et al. (2014) Hypoxia and hypoxia-inducible factor-1alpha provoke toll-like receptor signalling-induced inflammation in rheumatoid arthritis. Ann Rheum Dis 73:928–936
Sakai A, Hirano T, Okazaki R, et al. (1999) Large-dose ascorbic acid administration suppresses the development of arthritis in adjuvant-infected rats. Arch Orthop Trauma Surg 119:121–126
Davis RH, Rosenthal KY, Cesario LR, et al. (1990) Vitamin C influence on localized adjuvant arthritis. J Am Podiatr Med Assoc 80:414–418
Remans PH, Sont JK, Wagenaar LW, et al. (2004) Nutrient supplementation with polyunsaturated fatty acids and micronutrients in rheumatoid arthritis: clinical and biochemical effects. Eur J Clin Nutr 58:839–845
Mangge H, Hermann J, Schauenstein K (1999) Diet and rheumatoid arthritis—a review. Scand J Rheumatol 28:201–209
Skoldstam L, Hagfors L, Johansson G (2003) An experimental study of a Mediterranean diet intervention for patients with rheumatoid arthritis. Ann Rheum Dis 62:208–214
Aletaha D, Neogi T, Silman AJ, et al. (2010) 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European league against rheumatism collaborative initiative. Arthritis Rheum 62:2569–2581
Ebringer A, Wilson C (2000) HLA molecules, bacteria and autoimmunity. J Med Microbiol 49:305–311
Salminen E, Heikkila S, Poussa T, et al. (2002) Female patients tend to alter their diet following the diagnosis of rheumatoid arthritis and breast cancer. Prev Med 34:529–535
Kremer JM, Bigauoette J, Michalek AV, et al. (1985) Effects of manipulation of dietary fatty acids on clinical manifestations of rheumatoid arthritis. Lancet 1:184–187
Adam O, Beringer C, Kless T, et al. (2003) Anti-inflammatory effects of a low arachidonic acid diet and fish oil in patients with rheumatoid arthritis. Rheumatol Int 23:27–36
Geusens P, Wouters C, Nijs J, et al. (1994) Long-term effect of omega-3 fatty acid supplementation in active rheumatoid arthritis. A 12-month, double-blind, controlled study. Arthritis Rheum 37:824–829
Pedersen M, Stripp C, Klarlund M, et al. (2005) Diet and risk of rheumatoid arthritis in a prospective cohort. J Rheumatol 32:1249–1252
Benito-Garcia E, Feskanich D, Hu FB, et al. (2007) Protein, iron, and meat consumption and risk for rheumatoid arthritis: a prospective cohort study. Arthritis Res Ther 9:R16
Varma V, Yao-Borengasser A, Rasouli N, et al. (2007) Human visfatin expression: relationship to insulin sensitivity, intramyocel-lular lipids, and inflammation. J Clin Endocrinol Metab 92:666–672
Kawaguchi K, Maruyama H, Hasunuma R, et al. (2011) Suppression of inflammatory responses after onset of collagen-induced arthritis in mice by oral administration of the citrus flavanone naringin. Immunopharmacol Immunotoxicol 33:723–729
Oben J, Enonchong E, Kothari S, et al. (2009) Phellodendron and citrus extracts benefit joint health in osteoarthritis patients: a pilot, double-blind, placebo-controlled study. Nutr J 8:38
Lull C, Wichers HJ, Savelkoul HF (2005) Antiinflammatory and immunomodulating properties of fungal metabolites. Mediat Inflamm 2005:63–80
Yu S, Weaver V, Martin K, et al. (2009) The effects of whole mushrooms during inflammation. BMC Immunol 10:12
Fortin PR, Lew RA, Liang MH, et al. (1995) Validation of a meta-analysis: the effects of fish oil in rheumatoid arthritis. J Clin Epidemiol 48:1379–1390
Ariza-Ariza R, Mestanza-Peralta M, Cardiel MH (1998) Omega-3 fatty acids in rheumatoid arthritis: an overview. Semin Arthritis Rheum 27:366–370
Ward TL, Hosid S, Ioshikhes I, et al. (2013) Human milk metagenome: a functional capacity analysis. BMC Microbiol 13:116
Vaghef-Mehrabany E, Alipour B, Homayouni-Rad A, et al. (2014) Probiotic supplementation improves inflammatory status in patients with rheumatoid arthritis. Nutrition 30:430–435
Pineda Mde L, Thompson SF, Summers K, et al. (2011) A randomized, double-blinded, placebo-controlled pilot study of probiotics in active rheumatoid arthritis. Med Sci Monit 17:CR347–CR354
Kwon HK, Lee CG, So JS, et al. (2010) Generation of regulatory dendritic cells and CD4 + Foxp3+ T cells by probiotics administration suppresses immune disorders. Proc Natl Acad Sci U S A 107:2159–2164
Authors’ contributions
All authors were involved in drafting the article or revising it critically for important intellectual content, and all authors approved the final manuscript. Dr. He and Dr. Li had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Study conception and design: J. He, Y. Wang, J. Guo, and Z. Li.
Acquisition of data: Y. Jin, M. Feng, X. Zhang, X. Li, L. Su, A. Wang, L. Wu, X. Yu, L. Sun, X. Liu, Y. Wang, B. Jia, J. Li, J. Tao, F. Zhang, P. Yu, L. Cui, J. Yang, Z. Li, J. Xie, P. Wei, W. Sun, L. Gong, Y. Cheng, C. Huang, X. Wang, Y. Wang, H. Guo, H. Jin, X. Liu, G. Wang, Y. Wang, L. He, Y. Zhao, X. Li, and Y. Zhang.
Analysis and interpretation of data: J. He, Y. Wang, J. Guo, and Z. Li.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Disclosures
None.
Funding
This work was supported by the National Natural Science Foundation of China (No. 81373117 and No. 31270914) and the Beijing Municipal Science & Technology Commission (No. Z131107002213060).
Additional information
Jing He, Yu Wang and Min Feng have equally contributed to this work.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
He, J., Wang, Y., Feng, M. et al. Dietary intake and risk of rheumatoid arthritis—a cross section multicenter study. Clin Rheumatol 35, 2901–2908 (2016). https://doi.org/10.1007/s10067-016-3383-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-016-3383-x