
Abstract
The structure, interpretation and parameterization of classical compartment models as well as physiologically-based pharmacokinetic (PBPK) models for monoclonal antibody (mAb) disposition are very diverse, with no apparent consensus. In addition, there is a remarkable discrepancy between the simplicity of experimental plasma and tissue profiles and the complexity of published PBPK models. We present a simplified PBPK model based on an extravasation rate-limited tissue model with elimination potentially occurring from various tissues and plasma. Based on model reduction (lumping), we derive several classical compartment model structures that are consistent with the simplified PBPK model and experimental data. We show that a common interpretation of classical two-compartment models for mAb disposition—identifying the central compartment with the total plasma volume and the peripheral compartment with the interstitial space (or part of it)—is not consistent with current knowledge. Results are illustrated for the monoclonal antibodies 7E3 and T84.66 in mice.






Similar content being viewed by others

Notes
For the plasma compartment, the total plasma lymph flow L pla and the apparent total reflection coefficient σpla were defined as
$${L_{{\rm{pla}}}} = \sum\limits_{{\rm{tis}}} {{L_{{\rm{tis}}}}} \quad {\rm{and}}\quad {L_{{\rm{pla}}}}\cdot(1 - {\sigma _{{\rm{pla}}}}) = \sum\limits_{{\rm{tis}}} {{L_{{\rm{tis}}}}} \cdot(1 - {\sigma _{{\rm{tis}}}}).$$See [23] for naming, and below on how to exploit experimentally determined ABCexp to determine \(\widehat{K}_{\rm tis}\).
References
Keizer R, Huitema A, Schellens J, Beijnen J (2010) Clinical pharmacokinetics of therapeutic monoclonal antibodies. Clin Pharmacokinet 49:493
Vugmeyster Y, Xu X, Theil F, Khawli L, Leach M (2012) Pharmacokinetics and toxicology of therapeutic proteins: advances and challenges. World J Biol Chem 3(4):73
Jones H, Mayawala K, Poulin P (2013) Dose selection based on physiologically based pharmacokinetic (PBPK) approaches. AAPS J 15(2):377
Xiao J (2012) Pharmacokinetic models for FcRn-mediated IgG disposition. J Biomed Biotechnol 2012:282989
Baxter L, Zhu H, Mackensen D, Jain R (1994) Physiologically-based pharmacokinetic model for specific and nonspecific monoclonal antibodies and fragments in normal tissue and human tumor xenografts in nude mice. Cancer Res 54:1517
Ferl G, Wu M, Distefano AJ (2005) A predictive model of therapeutic monoclonal antibody dynamics and regulation by the neonatal Fc receptor (FcRn). Ann Biomed Eng 33(11):1640
Garg A, Balthasar J (2007) Physiologically-based pharmacokinetic (PBPK) model to predict IgG tissue kinetics in wild-type and FcRn-knockout mice. J Pharmacokinet Pharmacodyn 34:687
Davda J (2008) A physiologically based pharmacokinetic (PBPK) model to characterize and predict the disposition of monoclonal antibody CC49 and its single chain Fv constructs. Int Immunopharmacol 8:401
Urva S, Yang C, Balthasar J (2010) Physiologically based pharmacokinetic model for T84.66: a monoclonal anti-CEA antibody. J Pharm Sci 99(3):1582
Shah D, Betts A (2012) Towards a platform PBPK model to characterize the plasma and tissue disposition of monoclonal antibodies in preclinical species and human. J Pharmacokinet Pharmacodyn 39:67
Chen Y, Balthasar J (2012) Evaluation of a catenary PBPK model for predicting the in vivo disposition of mAbs engineered for high-affinity binding to FcRn. AAPS J 14(4):850
Lu J, Bruno R, Eppler S, Novotny W, Lum B, Gaudreault J (2008) Clinical pharmacokinetics of Bevacizumab in patients with solid tumors. Cancer Ther Pharmacol 62:779
Wiczling P, Rosenzweig M, Vaickus L, Jusko W (2010) Pharmacokinetics and pharmacodynamics of a chimeric/humanized anti-CD3 monoclonal antibody, Otelixizumab (TRX4), in subjects with psoriasis and with type 1 diabetes mellitus. J Clin Pharmacol 50:494
Dirks N, Nolting A, Kovar A, Meibohm B (2008) Population pharmacokinetics of cetuximab in patients with squamous cell carcinoma of the head and neck. J Clin Pharmacol 48:267
Azzopardi N, Lecomte T, Ternant D, Piller F, Ohresser M, Watier H, Gamelin E, Paintaud G (2010) Population pharmacokinetics and exposition-PFS relationship of cetuximab in metastatic colorectal cancer. Population Approach Group Meeting
Lammertsvan Bueren J, Bleeker W, Bogh H, Houtkamp M, Schuurman J, van de Winkel J, Parren P (2006) Effect of target dynamics on pharmacokinetics of a novel therapeutic antibody against the epidermal growth factor receptor: implications for the mechanisms of action. Cancer Res 66(15):7630
Mager D, Jusko W (2001) General pharmacokinetic model for drugs exhibiting target-mediated drug disposition. J Pharmacokinet Pharmacodyn 28:507
Mager D, Krzyzanski W (2005) Quasi-equilibrium pharmacokinetic model for drugs exhibiting target-mediated drug disposition. Pharm Res 22:1589
Gibiansky L, Gibiansky E, Kakkar T, Ma P (2008) Approximations of the target-mediated drug disposition model and identifiability of model parameters. J Pharmacokinet Pharmacodyn 35:573
Grimm H (2009) Gaining insights into the consequences of target-mediated drug disposition of monoclonal antibodies using quasi-steady-state approximations. J Pharmacokinet Pharmacodyn 36:407
Krippendorff B, Kuester K, Kloft C, Huisinga W (2009) Nonlinear pharmacokinetics of therapeutic proteins resulting from receptor mediated endocytosis. J Pharmacokinet Pharmacodyn 36:239
Krippendorff B, Oyarzn DHW (2012) Predicting the F(ab)-mediated effect of monoclonal antibodies in vivo by combining cell-level kinetic and pharmacokinetic modelling. J Pharmacokinet Pharmacodyn 39(2):125
Shah D, Betts A (2013) Antibody biodistribution coefficients: inferring tissue concentrations of monoclonal antibodies based on the plasma concentrations in several preclinical species and human. mAbs 5:2–297
Pilari S, Huisinga W (2010) Lumping of physiologically-based pharmacokinetic models and a mechanistic derivation of classical compartmental models. J Pharmacokinet Pharmacodyn 37:365405
Garg A (2007) Investigation of the role of FcRn in the absorption, distribution, and elimination of monoclonal antibodies. Ph.D. thesis, Faculty of the Graduate School of State University of New York at Buffalo
Hansen R, Balthasar J (2003) Pharmacokinetic/pharmacodynamic modeling of the effects of intravenous immunoglobulin on the disposition of antiplatelet antibodies in a rat model of immune thrombocytopenia. J Pharm Sci 92(6):1206
El-Masri H, Portier C (1998) Physiologically based pharmacokinetics model of primidone and its metabolites phenobarbital and phenylethylmalonamide in humans, rats, and mice. Drug Metab Dispos 26(6):585
Davies B, Morris T (1993) Physiological parameters in laboratory animals and humans. Pharm Res 10(7):1093
Kawai R, Lemaire M, Steimer J, Bruelisauer A, Niederberger W, Rowland M (1994) Physiologically based pharmacokinetic study on a cyclosporine derivative, SDZ IMM 125. J Pharmacokinet Pharmacodyn 22(5):327
Sarin H (2010) Physiologic upper limits of pore size of different blood capillary types and another perspective on the dual pore theory of microvascular permeability. J Angiogenesis Res 2:14
Covell D, Barbet J, Holton O, Black C, Parker R, Weinstein J (1986) Pharmacokinetics of monoclonal immunoglobulin G1, F(ab′)2, and Fab’ in mice. Cancer Res 46(8):3969
Brown R, Delp M, Lindstedt S, Rhomberg L, Beliles R (1997) Physiological parameter values for physiologically based pharmacokinetic models. Toxicol Ind Health 13(4):407
Lagarias J, Reeds JA, Wright MH, Wright PE (1998) Convergence properties of the nelder-mead simplex method in low dimensions. J Optim Theory Appl 9(1):112
Borvak J, Richardson J, Medesan C, Antohe F, Radu C, Simionescu C, Ghetie VWES (1998) Functional expression of the MHC class i-related receptor, FcRn, in endothelial cells of mice. Int Immunol 10(9):12891298
Akilesh S, Christianson G, Roopenian D, Shaw A (2007) Neonatal FcR expression in bone marrow-derived cells functions to protect serum IgG from catabolism. J Immunol 179:4580
Montoyo H, Vaccaro C, Hafner M, Ober R, Mueller W, Ward E (2009) Conditional deletion of the MHC class i-related receptor FcRn reveals the sites of IgG homeostasis in mice. PNAS 106(8):27882793
Ghetie V, Hubbard J, Kim MF, Tsen J-K, Lee Y, Ward E (1996) Abnormally short serum half-lives of igg in 2-microglobulin-deficient mice. Eur J Immunol 26:690
Rodgers T, Leahy D, Rowland M (2005) Physiologically based pharmacokinetic modeling 1: predicting the tissue distribution of moderate-to-strong bases. J Pharm Sci 94:1259
Stoop J, Zegers BJM, Sander PC, Ballieux RE (1969) Serum immunoglobulin levels in healthy children and adults. Clin Exp Immunol 4:101
EMEA (2013) Summary of product characteristics of cetuximab
EMEA (2012) Summary of product characteristics of infliximab
EMEA (2013) Summary of product characteristics of rituximab
EMEA (2013) Summary of product characteristics of trastuzumab
EMEA (2013) Summary of product characteristics of golimumab
EMEA (2013) Summary of product characteristics of tocilizumab
Huisinga W, Solms A, Fronton L, Pilari S (2012) Modeling inter-individual variability in physiologically-based pharmacokinetics and its link to mechanistic covariate modeling. CPT 1:e4
Cao Y, Balthasar JP, Jusko WJ (2013) Second-generation minimal physiologically-based pharmacokinetic model for monoclonal antibodies. J Pharmacokinet Pharmacodyn 40:597
Brambell F, Hemmings W, Morris I (1964) A theoretical model of gamma-globulin catabolism. Nat Biotechnol 203:1352
Junghans R, Anderson C (1996) The protection receptor for IgG catabolism is the β2-microglobulin-containing neonatal intestinal transport receptor. Proc Natl Acad Sci USA 93(11):5512
Acknowledgements
Ludivine Fronton and Sabine Pilari acknowledge financial support from the Graduate Research Training Program PharMetrX: Pharmacometrics & Computational Disease Modeling, Freie Universität Berlin and Universität Potsdam, Germany (http://www.PharMetrX.de). Fruitful discussions with the early DMPK, DMPK and M&S teams (F. Hoffmann-La Roche Ltd, pRED, Pharmaceutical Sciences, Basel, Switzerland) and Frank-Peter Theil and Jay Tibbits (UCB Pharma, Belgium) are kindly acknowledged.
Author information
Authors and Affiliations
Corresponding author
Appendices
Appendix: The role of FcRn and endogenous IgG in PBPK models of mAb disposition
From saturable IgG–FcRn interaction to linear mAb clearance
We illustrate that under commonly encountered (dosing) conditions, the clearance of mAbs in the endosomal space can be expected to be linear, regardless of the level of saturation of FcRn that protect mAb from degradation.
Denoting by IgGmAb and IgGendo the therapeutic and endogenous IgG concentrations in the endosomal space of endothelial cells, the resulting total IgG concentration was given by
In the endosomal space, free IgG binds to free FcRn with a dissociation constant K D forming an \({\rm IgG}\!:\!{\rm FcRn}\) complex. The relevance of FcRn stems from the fact that it protects IgG from catabolism [48]: While the complex is recycled to the interstitial and/or plasma space, free IgG is eventually catabolized in the lysosomes:
To study the IgG–mAb interaction in more detail, we denoted by FcRnu free FcRn, and by IgGu and IgGb the free and FcRn-bound IgG. Consequently, IgGu is the sum of the free endogenous and free therapeutic IgG. Two conservation relations IgG = IgGu + IgGb and FcRn = FcRnu + IgGb hold.
In the sequel, we made the assumption that the K D values of IgGendo and IgGmAb are comparable. This is a reasonable assumption for most mAbs—however, it does not hold for mAbs specifically engineered for high binding affinity to FcRn.
Binding processes are typically fast compared to the time-scale of other pharmacokinetic processes. Assuming a quasi-steady state for FcRn binding yielded \({\rm IgG}_{\rm u} \cdot {\rm FcRn}_{\rm u} = K_{\rm D} \cdot {\rm IgG}_{\rm b}\). Solving for the bound concentration and exploiting the conservation relations yielded
Exploiting again the second conservation relation, we obtained
and finally
with FcRneff = (FcRn − IgG − K D). This allowed us to determine the fraction unbound fuIgG based on Eq. (30) as
with FcRnu defined in Eq. (31). We defined the level of saturation of FcRn as
Figure 7 (left) shows the FcRn-saturation level as a function of the total IgG concentration, expressed in terms of units of total FcRn. We clearly identified two regimes: (i) for IgG lower than FcRn, the saturation level of FcRn appears to be linearly increasing with increasing IgG concentration; (ii) for IgG larger than total FcRn, the FcRn-saturation level appears to be 1. As shown below in "Theoretical derivation of FcRn saturation level and fraction unbound of mAb" section, this behavior can be theoretically justified based on the reasonable assumption that K D ≪ FcRn, i.e., that IgG has a very high affinity to FcRn. This assumption is in line with the physiological function of FcRn. For the mAb 7E3 in mice, we estimated the total FcRn concentration to be \(2.2 \cdot 10^5\) nM, while K D was reported to be 4.8 nM (see Table 1), thereby supporting the assumption K D ≪ FcRn.

FcRn saturation level (left) and fraction unbound of IgG (right) as a function of the total IgG concentration (stated in units of total FcRn). Due to the high affinity binding of IgG to FcRn, the FcRn saturation level growth practically linearly with IgG concentration, until FcRn is fully saturated. As a consequence, the fraction unbound fuIgG of IgG is practically zero until IgG concentration exceeds total FcRn concentration, when it follows the form fuIgG = 1 − FcRn/IgG. We choose FcRn = 105 nM and K D = 4.8 nM, in line with values reported in Table 1
As shown in Fig. 7 (right), the fraction unbound fuIgG also exhibited two regimes: (i) a phase of IgG concentration below FcRn, where fuIgG is almost zero, and (ii) a phase of hyperbolic increase for IgG above FcRn. This behavior can again be justified theoretically, as shown in the Appendix "Theoretical derivation of FcRn saturation level and fraction unbound of mAb" and summarized as
Without the underlying theoretical justification, such a model was proposed in [4], termed the cutoff model, based on some cutoff value ‘MAX’ (that is identical to total FcRn).
The above derivations have direct impact on modeling endosomal clearance and the FcRn-mediated salvage mechanism for a large number of mAbs. If the total IgG concentration is dominated by endogenous IgG and hardly perturbed by the administration of therapeutic IgG, i.e, IgGmAb ≪ IgGendo, which implies IgG ≈ IgGendo, then the fraction unbound of mAb is constant, i.e.,
Such a situation is quite common for many mAbs. In mice, the baseline concentration of endogenous plasma IgG1 is reported to be 14.7 μM in [26, 49]. In [4], the author showed that the administration of an i.v. bolus of 8 mg/kg therapeutic IgG (7E3) does not affect the overall endogenous plasma level of IgG. The same can be shown to hold true for many mAbs in human (see "Discussion" section). Under such conditions, the extent of saturation of FcRn and consequently the fraction unbound fumAb only depends on the endogenous IgG concentration; in other words, it is set by the endogenous IgG levels.
Theoretical derivation of FcRn saturation level and fraction unbound of mAb
The special form of the dependance of the
on the total IgG concentration can be theoretically justified from Eq. (31). To this end, we introduced the parameters
Due to very tight binding of endogenous IgG and mAb to FcRn, we made the reasonable assumption that \(\epsilon\) is very small, i.e., \(\epsilon\ll1\). For 7E3 in mice, we estimated \(\epsilon<5\cdot10^{-3}\) from Table 1. Dividing in Eq. (31) both sides by FcRn yielded the fraction unbound of FcRn:
or \({\rm FcRn}_{\rm u}/{\rm FcRn}=1/2\cdot(x+\sqrt{x^2+4\epsilon^2}).\) When \({\rm IgG}/{\rm FcRn}=(1-\epsilon)\), i.e., when (total) IgG concentration is approximately equal to the (total) FcRn concentration, it is x = 0 and therefore \({\rm FcRn}_{\rm u}/{\rm FcRn}=\epsilon\). Now, the larger the IgG concentration, the larger the bound fraction of FcRn and the smaller the unbound fraction of FcRn. Thus, \({\rm IgG}/{\rm FcRn}\geq(1-\epsilon)\) implies
This finally resulted in the lower bound on the FcRn saturation level:
for \({\rm IgG}/{\rm FcRn}\geq(1-\epsilon)\). For the upper bound for small IgG concentrations with \(\epsilon< x\), we used a simple estimate on the square-root term \(\sqrt{x^2+4\epsilon^2} < \sqrt{x^2+4x\epsilon}\) and applied the Taylor expansion to first order
for \(x\gg \epsilon\). This resulted in
On the other hand, by simply neglecting the \(4\epsilon^2\) term in the square root in Eq. (36), we obtained
From these two inequalities and Eq. (34) we finally obtained
for \(x\gg \epsilon,\) i.e., \({\rm IgG}/{\rm FcRn}\ll 1-\epsilon-\epsilon^2\). Taken together, Eqs. (38) and (42) theoretically justify the peculiar form of the FcRn-saturation level depicted in Fig. 7 (left).
The above derivation also allowed us to theoretically justify the dependence of the fraction unbound fuIgG on IgG, as shown in Fig. 7 (right). For \({\rm IgG}/{\rm FcRn}=(1-\epsilon)\) it is \({\rm FcRn}_{\rm u}/{\rm FcRn}=\epsilon\) as before, and
Since fuIgG decreases monotonically with decreasing IgG concentration, the bound \({\rm fu}_{\rm IgG}<\epsilon\) continues to hold for all \({\rm IgG}<(1-\epsilon){\rm FcRn}\). For larger IgG concentrations, we started from the relation
where we exploited IgGb = FcRnb = FcRn − FcRnu. For \({\rm IgG}/{\rm FcRn}\geq (1-\epsilon),\) we obtained with (37) the inequality
where the first inequality trivially follows from Eq. (44). Taken together, Eqs. (43) and (45) theoretically justify the peculiar form of the fraction unbound of IgG depicted in Fig. 7 (right).
Step-wise reduction of a detailed PBPK model of mAb disposition
Eliminating the need of endogenous IgG
The starting point of our simplified model was the tissue model of mAb disposition presented in [7, Fig. 2]. The tissue model comprised the vascular, endosomal and interstitial sub-compartments with the corresponding volumes V p, V e and V i. The following processes were considered: (i) transport into the interstitial space via convective transport through the paracellular pores in the endothelium (simplified two-pore model); (ii) convective transport via the lymph fluid from the interstitial space; (iii) uptake from the plasma and interstitial spaces into the endosomal compartments via fluid phase endocytosis; (iv) binding to FcRn in the endosomal compartments, (v) salvage of FcRn-bound complexes to the plasma and interstitial spaces; (vi) lysosomal degradation of the unbound species in the endosomal spaces. The corresponding system of differential equations for the rates of change of the (total) concentration in the vascular space C p, in the endosomal space C e and in the interstitial space C i are given by
with the parameters having the following meaning: Q and L denoted the plasma and lymph flows, \({\rm \sigma_{\rm vas}}\) and \({\rm \sigma_{\rm lymph}}\) denoted the vascular and lymphatic reflection coefficients, k in denoted the endosomal uptake rate constant, k out denoted the recirculation rate constant, and FR denoted the recirculation fraction of bound antibody from the endosomal into the vascular space. The unbound antibody in the endosomal space was subject to elimination following a linear clearance denoted by CLe. The fraction unbound fu in the endosome was defined as in Eq. (32).
The authors in [7] explicitly considered endogenous IgG in their model—in addition to therapeutic IgG to account for the competition for binding of mAb and endogenous IgG to FcRn. Based on the observation preceding Eq. (33) and thereon based derivations, we could greatly simplify the above tissue model by only implicitly considering endogenous IgG. We indeed assumed that the fraction unbound of mAb in the endosome is constant. Therefore, we defined the total FcRn-mediated export flow and the endosomal intrinsic clearance as
This was the basis for an intermediate complexcity of a PBPK model for mAbs disposition.
An intermediate complexity of PBPK models for mAb disposition
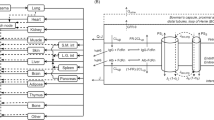
The intermediate PBPK model comprised 32 compartments representing the most relevant anatomical spaces involved in mAb disposition (see Fig. 8): venous (ven) and arterial (art) plasma as well as the vascular plasma (p), endosomal (e) and interstitial (i) spaces of ten tissues. In addition to the process at the tissue level, the model incorporated the distribution of mAb via the plasma flow and the convective transport with the lymph flow from the interstitial spaces back into the plasma circulation. The rates of change of all concentrations are given by
For all tissues except vein, artery, liver and lung, the inflowing concentration C in was given by C in, tis = C art; for lung, it was \(C_{{\rm in},{\rm lun}}=C_{\rm ven}\). For vein, it was
with tis = adi, bon, hea, kid, liv, mus, ski. For liver, it was
with tis = gut, spl. The mAb was administered via an i.v. bolus infusion. For the vein, the initial condition of the above system of differential equations was set to
while we set C cmt(0) = 0 for all other compartments ’cmt’.

Detailed PBPK model structure. Top structure of the PBPK model for mAbs. Organs, tissues and plasma spaces are interconnected by the plasma flow (red and blue solid arrows) and the lymphatic system (green dashed arrows). Bottom detailed organ model comprising a plasma compartment, the endosomal and the interstitial spaces. Q and L represent the plasma and lymph flow, \({\rm \sigma_{\rm vas}}\) and \({\rm \sigma_{\rm lymph}}\) denote the vascular and lymphatic reflection coefficients, k in is the rate of uptake of mAb from the plasma or interstitial space into the endosomal space. The parameter k out is the recycling rate constant of mAb from the endosomal space (with a fraction FR recycled into the vascular space), while fuCLe denotes its linear clearance in the endosomal space
Lumping all (vascular) plasma spaces and tissue sub-compartments
The following reduction was justified based on time-scale arguments. To this end, we considered the generic ODE for the rate of change of the concentration C cmt of some compartment ‘cmt’ with inflow Q inflow and outflow Q outflow:
The response time τcmt—i.e., the time scale, on which the compartment concentration responses to changes in the inflowing concentration C in—is given by
Hence, small compartments or compartments with large outflow response quickly to changes in the inflow. Of note, the inflow Q inflow does only influence the concentration levels C cmt and its steady state concentration, but has no impact on the response time.
In view of the systems of ODEs Eqs. (51–54), we identified three groups of compartments with different response times (supported by parameters values published in [7–10] and physiological insight):
-
Fast: Arterial and venous plasma and peripheral plasma of all tissues with response times
$$\tau_{\rm art} = \frac{\ln(2)}{Q_{\rm art}/V_{\rm art}}; \quad \tau_{\rm ven} = \frac{\ln(2)}{Q_{\rm ven}/V_{\rm ven}},$$and
$$\tau_{{\rm p},{\rm tis}} = \frac{\ln(2)}{(Q_{\rm tis}-L_{\rm tis})/V_{{\rm p},{\rm tis}}}.$$We define τpla as the average of the above response times.
-
Intermediate: The interstitial space of all tissues, with response times
$$\tau_{\rm i} < \frac{\ln(2)}{(1-{\rm \sigma_{\rm lymph}})L_{\rm tis}/V_{\rm i}}.$$We define τint as the average of the above response times. Comparison to plasma response time: V pla and V i are roughly of the same order of magnitude (e.g. [5]), while L tis is roughly two-orders of magnitude smaller than Q tis, and \((1-{\rm \sigma_{\rm lymph}})=0.8\) [7]. Consequently, plasma & vascular compartments response is approximately two-orders of magnitude faster than the interstitial compartments, i.e., τpla ≪ τint. Of note, the much slower inflow corresponding to \((1-{\rm \sigma_{\rm vas}})L_{\rm tis}\) does not influence the response time, it only influences the interstitial concentration levels.
-
Slow: The endosomal space of all tissues, with response times
$$\tau_{\rm e} < \frac{\ln(2)}{(Q_{{\rm out},{\rm tis}}+{\rm CLint}_{\rm e})/V_{\rm e}} \leq \frac{\ln(2)}{Q_{{\rm out},{\rm tis}}/V_{\rm e}}.$$We define τend as the average of the above response times. According to [7], V e is approximately two-orders of magnitude smaller than V i, while at the same time Q out, tis is five orders of magnitude smaller than Q tis and therefore three orders of magnitude smaller than L tis. Consequently, interstitial compartments response is approximately one order of magnitude faster than the endosomal compartments, i.e., τint < τend.
The above time-scale considerations suggest to lump together arterial and venous plasma and all peripheral plasma spaces, resulting in a lumped plasma compartment with total plasma volume V pla and plasma concentration defined by
Moreover, due to the larger uncertainty of parameters related to the endosomal space, we decided to lump together the interstitial and endosomal space of each tissue. For easier comparison to experimental data, we also included the intracellular space with volume V c, and defined the tissue volume by V tis = V i + V e + V c and the tissue concentration by
Since the mAb—in the absence of a target—does not distribute in the intracellular space, it is C c = 0.
We finally derived the ODEs describing the rate of change of C pla and C tis in the different tissues. For plasma, we obtained
We subsequently exploited \(C_{\rm pla}=C_{\rm ven}=C_{\rm art}=C_{{\rm p},{\rm tis}}\) and made the following assumptions, to derive the final equation for plasma: (i) Since it is difficult to distinguish between the two-pore-related and the fluid-phase endocytotic part of the vascular extravasation, i.e., \(L_{\rm tis} (1-{\rm \sigma_{\rm vas}})\) versus \(V_{{\rm p},{\rm tis}} k_{\rm in}\), we only used a single term (\(L_{\rm tis} (1-\sigma_{\rm tis})\)) and introduced an effective lumped reflection coefficient σtis such that
Further, (ii) since we lump all tissue sub-compartments, we assumed that \(C_{\rm e}\)and \(C_{\rm i}\) are multiples of the lumped concentration C tis, i.e. C e = α C tis and \(C_{\rm i}=\beta C_{\rm tis}\). Writing moreover \(Q_{{\rm out},{\rm tis}}\) as a fraction δ of the lymph flow L tis yielded
and allowed us to define the tissue partition coefficient K tis as
As a consequence, we obtained the final ODE for the rate of change of the plasma concentration
which is identical to Eq. (2). For the tissue concentration C tis we obtained
Defining the intrinsic tissue clearance \({\rm CLint}_{\rm tis} = {\rm CLint}_{\rm e}\cdot\alpha\) and using the same assumptions and arguments as above, we obtained
which is identical to Eq. (1). In summary, we derived our simplified PBPK model given in Eqs. (1–2) from a much more detailed PBPK model by considering time-scale separation and additional well-grounded assumptions. The resulting number of equations was reduced by a factor of approximately 6 and 3 in comparison to [7] and [10], respectively.
Derivation of the ODEs of the lumped compartments
Based on Eq. (13), we derived the ODE describing the rate of change of the lumped concentrations C L with L = {\({\rm tis}_1, \ldots, {\rm tis}_k\)}. To this end, we first established the relation between the lumped concentration C L and some tissue concentrations C tis with \({\rm tis}\in{\rm L}\). Starting from Eq. (13), we obtained
where we used in the third line the lumping criterion \(C_{\rm tis}/((1-\sigma_{\rm tis}) \cdot\widehat{K}_{\rm tis}) = C_{{\rm tis}_i}/((1-\sigma_{{\rm tis}_i})\cdot \widehat{K}_{{\rm tis}_i})\) for \({\rm tis}\in{\rm L}\) and i = 1,…, k; and in the last line we used Eq. (14). Rearranging the above equation yielded
For the plasma compartment, this specifically read
For all compartments except for the central compartment, we obtained
where we exploited Eq. (64) in the third line. Thus
For the central compartment, we obtained
where we exploited in particular Eqs. (12) and (16). These equations are the foundation for the derivation of lumped compartment models in the next section.
Rights and permissions
About this article
Cite this article
Fronton, L., Pilari, S. & Huisinga, W. Monoclonal antibody disposition: a simplified PBPK model and its implications for the derivation and interpretation of classical compartment models. J Pharmacokinet Pharmacodyn 41, 87–107 (2014). https://doi.org/10.1007/s10928-014-9349-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10928-014-9349-1