
Abstract
Background
Recent estimates suggest the prevalence of non-cystic fibrosis bronchiectasis (NCFB) may be increasing in the US. The objective of this study was to determine the current economic burden of NCFB compared with non-NCFB controls in the first year after diagnosis within a commercially enrolled US population.
Methods
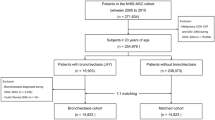
A retrospective matched cross-sectional case control (1:3) study design was used. Data were derived from MarketScan® Commercial Claims and Encounters Database, which captures all patient-level demographic data and all medical and pharmacy claims during the period 1 January 2005 to 31 December 2009. NCFB patients were identified using ICD-9 codes 494.0 and 494.1. Individuals with medical claims for cystic fibrosis or chronic obstructive pulmonary disease were excluded. Incremental burden of NCFB was estimated for overall and respiratory-related expenditures using multivariate regression models which adjusted for baseline characteristics and healthcare resource utilization. All demographic characteristics and economic outcomes were ascertained in 12 months before (baseline period) and 12 months after (follow-up) index event, which was defined as the first bronchiectasis-related medical event. Non-parametric bootstrap technique was used to calculate the 95 % confidence limits for the adjusted estimate. All costs are inflation-adjusted to a baseline year of 2009 using the consumer price index. All statistical tests were conducted using SAS 9.2 and STATA 12.0.
Results
The study sample used for healthcare burden analyses had 9,146 cases and 27,438 matched controls. The majority of the sample was between the ages of 45–64 years old and 64 % were female. A greater proportion of cases than controls had an increase from baseline to follow-up in both total (49 vs 40 %) and respiratory-related costs (57 vs 25 %). The average increase in overall and respiratory-related costs compared with controls after adjusting for differences in baseline characteristics was US$2,319 (95 % CI 1,872–2,765) and US$1,607 (95 % CI 1,406–1,809), respectively. The primary driver for this increment was increase in outpatient visits of approximately 2 overall and 1.6 respiratory-related visits per patient per year, which translated to US$1,730 (95 % CI 1,332–2,127) and US$1,253 (95 % CI 1,097–1,408), respectively.
Conclusion
This study found that the cost of managing NCFB in the first year within a commercially enrolled population may be burdensome. Compared with previously published estimates in the literature, the burden of NCFB may be also increasing.


Similar content being viewed by others

References
Evans DF, Bara AI, Greenstone M. Prolonged antibiotics for purulent bronchiectasis. Cochrane Database Syst Rev. 2003;4:CD001392.
Ilowite J, Spiegler P, Chawala S. Bronchiectasis: new findings in the pathogenesis and treatment of this disease. Curr Opin Infect Dis. 2008;21(2):163–7.
Barker AF. Bronchiectasis. N Eng J Med. 2002;346(18):1383–93.
O’Donnell AE. Bronchiectasis. Chest. 2008;134(4):815–23.
Zoumot Z, Wilson R. Respiratory infection in noncystic fibrosis bronchiectasis. Curr Opin Infect Dis. 2010;23(2):165–70.
Martinez-Garcia MA, Soler-Cataluna JJ, Perpina-Tordera M, et al. Factors associated with lung function decline in adult patients with stable non-cystic fibrosis bronchiectasis. Chest. 2007;132(5):1565–72.
Prasad M, Tino G. Bronchiectasis, part 2: management. J Respir Dis. 2008;29(1):20–5.
Seitz AE, Olivier KN, Sreiner CA, et al. Trends and burden of bronchiectasis-associated hospitalizations in the United States, 1993–2006. Chest. 2010;138(4):944–9.
Weycker D, Edelsberg J, Oster G, et al. Prevalence and economic burden of bronchiectasis. Clin Pulm Med. 2005;12(4):205–9.
Metersky ML. New treatment options for bronchiectasis. Ther Adv Respir Dis. 2010;4(2):93–9.
Seitz AE, Olivier KN, Adjemian J, et al. Trends in bronchiectasis among medicare beneficiaries in the United States, 2000–2007. Chest. 2012;142(2):432–9.
Patel IS, Vlahos I, Wilkinson TMA, et al. Bronchiectasis, exacerbation indices, and inflammation in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2004;170(4):400–7.
O’Brian C, Guest PJ, Hill SL, et al. Physiological and radiological characterization of patients diagnosed with chronic obstructive pulmonary disease in primary care. Thorax. 2000;55(8):635–42.
Martinez-Garcia MA, Soler-Cataluna JJ, Donat Sanz Y, et al. Factors associated with bronchiectasis in patients with COPD. Chest. 2011;140(5):1130–7.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613–9.
Acknowledgment
The authors would like to thank Bridget Banas for assistance in writing this manuscript.
Funding source
Funding was provided by Bayer HealthCare Pharmaceuticals Inc., Wayne, NJ, USA.
Conflict of Interest
All authors are employed at Bayer Health Care Pharmaceuticals, which has R&D investment in anti-infectives. No other conflicts of interest noted.
Authors’ Contribution
V. N. Joish contributed to the study design, methods, results interpretation and editorial support and is the overall guarantor of this manuscript. M. Spilsbury contributed to the study objectives, methods, results interpretation and editorial support. E. Operschall contributed to the study objectives, methods, results interpretation and editorial support. B. Luong contributed to the study objectives, results interpretation and editorial support. S. Boklage was responsible for the statistical analyses plan and data analytics.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Joish, V.N., Spilsbury-Cantalupo, M., Operschall, E. et al. Economic Burden of Non-Cystic Fibrosis Bronchiectasis in the First Year after Diagnosis from A US Health Plan Perspective. Appl Health Econ Health Policy 11, 299–304 (2013). https://doi.org/10.1007/s40258-013-0027-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40258-013-0027-z